Embryo screening is a lightning rod for constructive criticism, most recently in the context of Orchid’s embryo screening for predisposition to severe mental health disease, namely Schizophrenia (Orchid screens for both monogenic and polygenic disease)[1].
I want to talk about one quote which specifically bothers me:
To me, it’s not.
The point of studying the genetics of disease is so children born in 2024 can be healthier, happier, and live longer than I will. Modern medicine is an incredibly laudable enterprise which has saved and will ad infinitum save millions of lives a year, even in a world where every embryo was screened for genetic disease. But disease prevention via embryo screening isn’t comparable to pharmaceuticals and as a parent I think it’s crazy to equate the the two [2].
Preventing a disease by selecting an embryo with lower genetic predisposition to disease, or which is free of a monogenic disorder, means that if you succeed [3], your child doesn’t have the disease. Successfully treating a disease via therapeutics means your child is free of disease as long as the medical system and pharmaceutical industry is functioning at high efficiency.
And I mean, it mostly has. If I was writing this post in 2019, there was a case to be zealously bullish on globalism, to believe we had passed the event horizon of interconnectedness and international trade would grow stronger until it sustained itself completely independent of the mundane politics of disease and fuel prices and cargo ships being blown up by ballistic missiles, but the pandemic cracked that fantasy and anyone who tried to buy toilet paper or cars in 2020 knows that supply chains work until they don’t.
But it’s obvious now that international trade is fragile when actual history happens. That may be a reasonable tradeoff; if a global pandemic cuts car imports in half, it’s inconvenient but you drive to Walmart in a 1995 Sonoma instead of a 2023 Kia to buy domestic wonderbread and somehow muddle through.
But if a global pandemic cuts insulin production in half, your diabetic child dies.
Medicine being unavailable for good, bad, or surprise reasons is not a hypothetical thing, it’s something that all normal people on prescriptions know and are terrified of:
- Diabetes is one of the best-understood and managed chronic diseases, but that management (esp for Type 1 diabetes) requires insulin. When the pandemic started and supply chains collapsed, millions of people were afraid that they would be unable to refill prescriptions.
- ADHD is an extremely well-understood disease, whose management requires medication. For more than a year, there has been a critical shortage of Adderall manufacturing, and nobody is close to figuring out why, much less fixing it.
- When Ivermectin supplies got shanghaied by mobs using it as moonshine COVID-19 therapeutics, people who genuinely needed it to treat Arthritis got completely shafted by supply shortages.
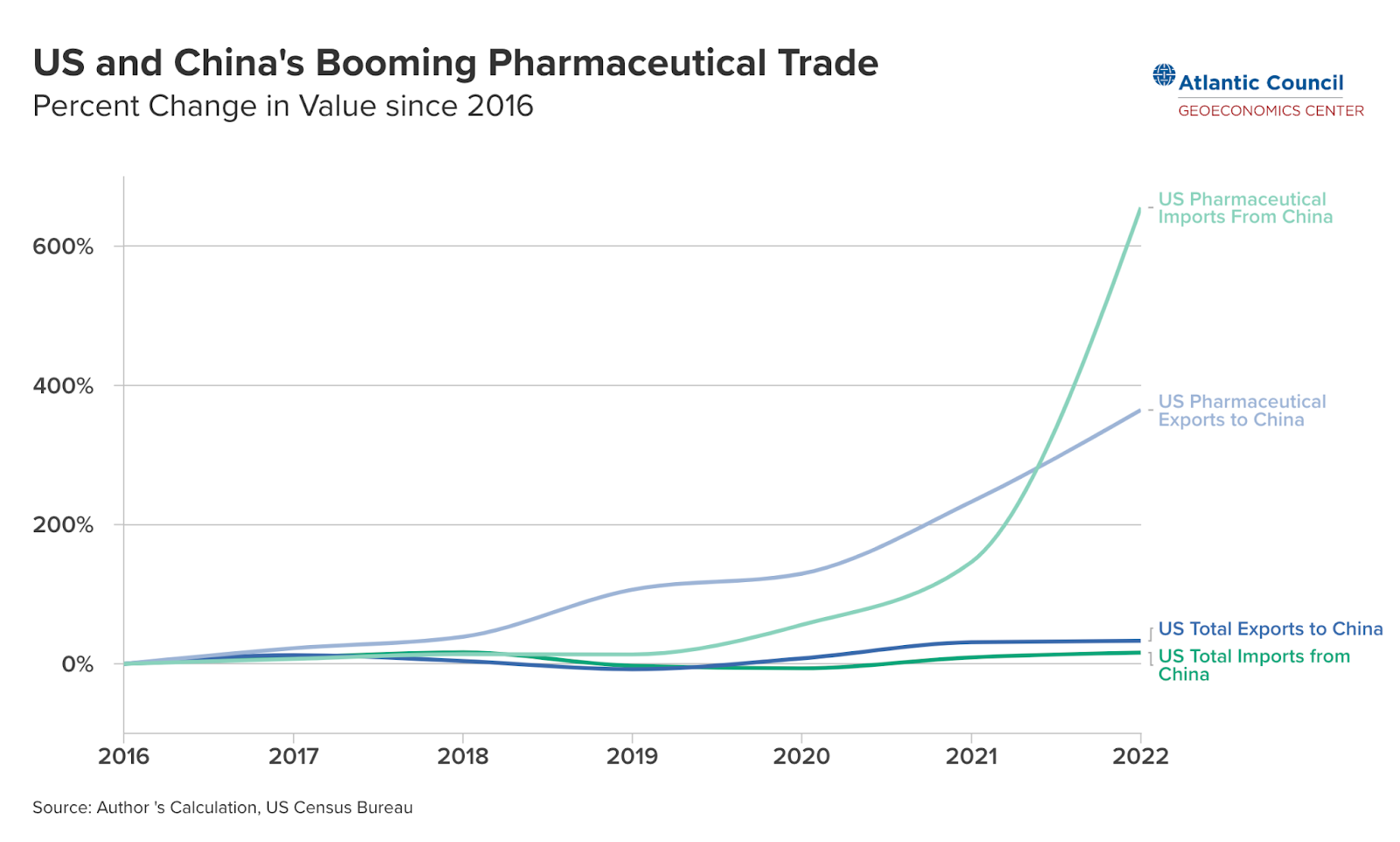
- An increasing % of US pharmaceuticals are either imported directly from China or rely on imported ingredients. Global trade is fragile, and there are a thousand possible conflicts even short of a hot war that would kneecap this supply. Cheap consumer imports are easily substitutable, drugs are not.
- Sometimes drugs just disappear! It might be regulatory or because your disease is rare and unprofitable or maybe they lost a patent case. It’s unlikely that drugs for major, common diseases disappear altogether, but if you have a specific rare disease, good luck!
- The good news? We have a pharmaceutical for severe allergies, Epinephrine! The bad news? EpiPens that used to go for $100 are now $600! And they expire every year! Deal with it!
We live in a hyperconnected world, we’re obviously not walking that back, even the most intense offgrid survivalists can maybe set themselves up for a decade of self-sufficiency before their solar panels degrade, water pumps fail and they have to reconnect with civilization or die of dysentery. I get it.
But I can’t put myself in the mindset of wanting to bind their children to the good grace and fortunes of the multinational pharmaceutical-industrial complex. For daily medication! The most charitable way to frame this statement is to say, it’s a statement from someone who has never been let down by the medical system, and has confidence that the engine will spit out pills at nominal capacity for the rest of our natural lives.
And maybe it will! But I think I speak for the vast majority of parents when I say I would rather not bet my children on it.
Appendix:
The more mundane criticism here is, couples have been using monogenic preimplantation testing (PGT-M) for decades, and nobody is telling parents they are immoral to screen their children for deafness or Huntington’s disease. Why is it ethically repugnant to do the same for mental health? I genuinely have trouble playing devil’s advocate on this point. The only possibilities I can think of:
- Schizophrenia isn’t a “real” disease to the critics. Maybe they are more open to screening for cancer and heart disease predisposition? I doubt this, because this line of criticism comes from mental health researchers!
- Lack of confidence in the strength of the datasets being used to construct Schizophrenia predisposition scores. But if you think that, say it! That’s not an indictment of the ethics, it’s a criticism of the data.
What am I missing here?
[1] I lead engineering at Orchid
[2] Gene therapy is the obvious exception here; gene therapy is incredibly promising and I hope it takes off. However it’s hard to imagine gene therapy in the near-term moving the needle on rare disease much less polygenic disease.
[3] Polygenic predispositions are of course a thousand miles away from a guarantee. The science improves each year, but for now you’re just weighting the dice.

As a Genetic Counselor by training, I want to say that I’m largely on your side on these issues. However, I must tell you one thing you are missing is that handwringing over monogenic prenatal/preimplantation screening/testing exists at a much higher level then this post makes it seem like you think it does.
There are absolutely people in the deaf community who will tell you that you are acting immorally if you choose to screen for common causes of deafness. See this study (https://www.jstor.org/stable/20696690) of hearing children of deaf adults where “60% believed that reproductive technologies, when used to select for or against deafness, should not be available to the community” and if you’re double taking at the idea of selection FOR deafness realize that there is a non-trivial portion of the deaf community who want to use PGD for exactly that purpose. See https://pubmed.ncbi.nlm.nih.gov/31542873/ for discussion. Genuinely difficult for me to think of a worse example you could have plucked than deafness to claim ‘no one’ will morally condemn you for screening against it (the dwarfism/LP community would probably be a close second worst). Huntington’s is far cleaner example, but given that it is largely adult onset you could probably still find someone to condemn you for it. For future use, Tay-Sachs is really what you’re looking for. Infantile onset, completely devastating, and screening/pgd has been eagerly embraced by the community most affected, Ashkenazi Jews.
Even though it is not monogenic, Down syndrome is essentially mono causal (let’s just ignore non-trisomy 21 causes like unbalanced translocations being carried by parents for now) and can generally be detected similarly to monogenic conditions. We’ve been hugely successful at identifying cases where Down syndrome will occur prenatally and most couples choose to terminate when it is identified, but you’d be wrong to assume there isn’t a group judging these couples. See https://www.theatlantic.com/magazine/archive/2020/12/the-last-children-of-down-syndrome/616928/ and https://www.statnews.com/2018/05/18/down-syndrome-prenatal-testing/ for two examples.
And really everything I’ve linked so far is moderate in tone compared to some of the writing/rhetoric I’ve seen out of academics who focus on disability studies (especially when the academics themselves are disabled), I won’t track down/link the most egregious examples I’ve seen because it’s late and I don’t feel like getting that angry before bed. I hope I’ve opened your eyes to the fact that debates about testing and screening for monogenic disease are still occurring and trying to move on to discussing the ethics of screening for polygenetic disorders without at least being aware of that is going to leave your arguments incomplete.
Oh yeah, thanks for the note. I’m definitely aware that there are communities upset about genetic screening even for clear monogenic disorders. I should clarify when I say “nobody is telling parents they are immoral to screen their children for deafness or Huntington’s disease”, I am really getting at the experience of prospective parents:
– Genetic counselors are not warning parents against carrier screening. At least not mainstream ones.
– Bioethicists have mostly ceded that screening for standard gene lists is OK (although the fringe tail here is long)
As opposed to polygenic screening, where parents are fighting an uphill battle to get their providers to order PGT-P on their behalf, even when there is a clear family history of disease.
But yeah, I don’t want to research too deep here or I’m going to go totally insane. I think they are losing, but it’s insane we have to debate this stuff in the first place.